

Cart (0 Items)
Your cart is currently empty.
View ProductsIt looks like you are visiting from outside the EU. Switch to the US version to see local pricing in USD and local shipping.
Switch to US ($) Antibody-drug conjugates
Antibody-drug conjugates
 Thomas Meyer
Thomas Meyer
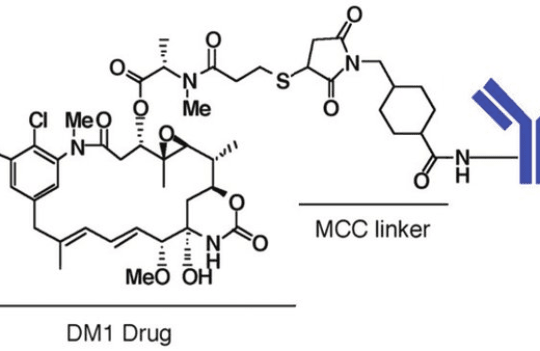
Antibody-drug conjugates (ADCs) are currently recognized as potent anti-cancer therapies targeting both solid tumors and hematological malignancies with high effectiveness. The conventional structure of ADCs consists of potent cytotoxic agents attached to an antibody carrier via a chemical linker. Dozens of ADCs have received marketing approval by the FDA in recent years and many more are currently under active clinical development.
The advantages of these therapies stem from their high target specificity allied to the potency of their toxic payloads. By acting synergistically, ADCs overcome the most common limitations of immunotherapies and chemotherapies alone – the lack of potency and excess of toxicity, respectively. With the development of new linker chemistry, conjugation technologies, and the use of new payloads, ADCs are expected to bring novel therapeutic breakthroughs in the coming decades.
ADCs can be defined as advanced delivery systems where the antibody is responsible for binding a specific surface cell receptor and the payload for exerting a biological effect. The major mechanism of action of ADCs can be described as follows:
Because this mechanism requires the efficient internalization of intact ADC molecules, linkers have been engineered for enhanced safety and targets have been selected following strict criteria. The ideal targets of ADC therapies can be summarized as follows:
This has prompted the development of a robust generation of ADCs with enhanced efficiency. However, this mechanism of action has proved to be highly efficient against hematological tumors and highly limited when targeting solid tumors. In general, ADCs diffuse poorly in solid tumors due to the antigen barrier imposed by peripheral cancer cells and the large size of the ADC molecule. Next-generation ADCs have emerged with the purpose of better countering these limitations.
Currently, many ADCs have been designed to favor the use of highly efficient and specific linkers, able to release the payload in the tumor microenvironment and forgo the need for internalization. By releasing the cargo on the extracellular space, the small cytotoxic agents are free to diffuse quickly through the cell membrane and target both antigen-positive and antigen-negative cancer cells (bystander effect). This is a crucial advantage due to the heterogeneity of solid tumors and their propensity for developing resistance by mutation of surface cell receptors.
Dozens of ADC therapeutics have reached the clinic since the approval of Mylotarg in 2000. Currently, many more ADCs populate the clinical pipeline promising to bring new and ground-breaking tools to our anti-cancer arsenal within the next decades. Historically, ADC therapies have focused on highly abundant surface cell receptors including:
In recent years, there has been an increased interest in developing ADCs targeting solid tumors. In this context, several promising markers are currently being investigated:
ADC therapies face three important challenges: limited efficacy against solid tumors, tumor-initiating cells (TICs), and senescent cells. Eradicating these cells while keeping systemic toxicity low is key to improving the overall prognostics of many types of cancer. With this purpose in mind, researchers are actively exploring alternative structures and strategies for therapeutic ADC development:
You could also be interested in:
Join our email list to receive exclusive content featuring the most interesting industry and research news, biologics development tips pieced together by experts, res, company news, and exclusive limited-offers. Join a community of 80,000 subscribers and save up to 30% on your first order.